The scope of application of massage tables today is really wide. In addition to the medical institutions themselves, these include beauty salons, fitness centers, and specialized massage rooms... Therefore, the question the right choice the table is now key. The relaxation and comfort of your patients, as well as the performance of your massage therapists, depends on a well-chosen couch.
At first glance, the design of the table is simple; models from different manufacturers often seem similar in appearance, but in fact, to choose a high-quality massage table, you need to take into account some features.
In order for a table to serve faithfully for a long time, it must be easy to use, safe, resistant to wear and possible external influences. For example, the table material should not be afraid of oils used in aroma massage sessions. The surface should be of medium softness - a hard table can cause discomfort to the patient, and too soft can make it difficult to carry out the massage as necessary. A large number of sections and accessories will allow you to “customize” the table to almost any wishes of the massage therapist and patients. Best option massage table – three-section with headrest and armrests. It's best if the accessories are already included. Tables come with mechanical and electrically adjustable– the main thing is that it is smooth and stepless. Almost all models have eyelets - holes for the face. In many models they are closed with special plugs. It's definitely more convenient.
An important issue in choosing is the factor of its reliability. After all, it must withstand peak loads reaching up to 200 kg! Leading brands make their products from durable aluminum frames.
The color of the table also matters. Many models of massage tables are available in several versions color scheme, so you can always choose a table that harmonizes with the interior.
How to choose a portable table?
Separately, you need to dwell on the features of choosing a portable massage table. IN Lately This type is becoming increasingly popular. The massage therapist is no longer tied to the massage parlor; he can perform massage on the patient’s premises, at a time convenient for him. When choosing a portable table, of course, first of all, other things being equal, the folded dimensions and weight matter. Usually it does not exceed 15 kg. To strengthen the structure, folding tables use a cable system, which allows them to withstand heavy weight. The quality of the connecting fittings and fasteners is also important so that over time there is no play or squeaking when using the table. A useful addition to folding table There will also be a special carrying bag - reputable manufacturers have it included in the kit.
Everyone knows about the delights of massage, but few people know about the difficulties of performing this procedure. In fact, massage is a very difficult and tedious job, even for experienced and trained professionals. One can only imagine how much pressure a massage therapist feels when doing massage all day long.
The main tool of the massage therapist is the table. Exactly correct adjustment massage table affects the preservation of health and increased efficiency of the massage therapist. Before you begin performing massage procedures, you need to understand the rules for organizing workplace ergonomics, i.e. massage table. The height of the massage table can vary from 60 to 90 cm. this parameter the most important, and its adjustment should be given Special attention.
What table height is considered correct?
It cannot be said that 60 or 80 centimeters will be a suitable height. It all depends on the anthropometric size of the specialist. Moreover, height plays a role, but the length of the massage therapist’s arms.
So, approach the table from the side. Stand so that your arms hang freely along your body. The ideal height would be when the hand clenched into a fist touches the surface of the table.
In addition to this measurement, you need to take into account the parameters of the person who is to be massaged. For example, massaging a patient with a solid build will require greater intensity of movement, and therefore, a lower seating position of the table will allow for more space for activity. In general, everyone sets up their workplace as it suits them, however, do not forget about the rules.
Let's look at the variations in height changes on the tables of the American company US Medica Sakura and Master. Both tables have long established themselves as perfect tool for professional massage. The difference between these tables lies in the design solutions. The Master is built in precious wood, while the Sakura is built on a tubular frame made of high-strength steel. We will not describe here the unreliability and ergonomic qualities of these tables; they are impeccable. We are interested in the possibility of customizing these tables for the master.
So, Sakura has an incredible range, the adjustment of which allows height changes from 59 to 84 cm. This indicator indicates almost comprehensive adjustment. The Sakura massage table will “adapt” to any person and any task. The height is adjusted by extending the legs and secured with screw-on buttons. There are two buttons on each leg, which gives the structure additional reliability and stability.
It boasts no less outstanding functionality a massage table Master. Its design provides a slightly different range of height adjustment (62-88 cm), but at the same time, these are the height parameters that are most in demand. The Master table height adjustment mechanism is presented in the form of a telescopic system, which makes adjustment as quick and practical as possible.
Remember, all settings are completely individual. At the same time, it is better to immediately develop the right habit; subsequently, this will have a beneficial effect on overall performance, and, consequently, the effectiveness of the procedures performed.
Massage is used for rehabilitation, prolonging youth and solving problems with the musculoskeletal system. From the patient's point of view, the massage table helps ensure comfort throughout the entire procedure. However, this piece of furniture is needed to an even greater extent by doctors - massage therapists and chiropractors. Considering the diversity of today's assortment medical furniture, it makes sense to talk about the principles of good choice.
Couch or professional massage table?
A price comparison shows that a regular couch, which many people use for massage, is cheaper than a massage table. As a result, the classic question arises: “Why pay more?” However, there are reasons for this - primarily among doctors who value their image and the comfort of their clients. Agree, this is a more powerful argument than diplomas and certificates.
When the patient is able to relax better, healing effect massage intensifies. In addition, patients have different anthropometric parameters. Massage tables adapt well to a person’s height and weight, which cannot be said about a couch. Another factor is to facilitate the work of a massage therapist, who is exposed to significant stress during the day. The work of engineers and clinical trials make the designs more ergonomic.
How not to make a mistake when choosing a manufacturer?
 Since there are many types of massage, it is not surprising that there are many manufacturing companies. Each of them talks about its advantages and makes arguments that are logical at first glance. However, objectively speaking, the recognized leaders of the world market are 2 brands - US MEDICA and YAMAGUCHI.
Since there are many types of massage, it is not surprising that there are many manufacturing companies. Each of them talks about its advantages and makes arguments that are logical at first glance. However, objectively speaking, the recognized leaders of the world market are 2 brands - US MEDICA and YAMAGUCHI.
US Medica produces the most complete line of massage tables, which is attractive in terms of functionality, price and quality. The Japanese manufacturer YAMAGUCHI focuses on versatility, and makes both stationary and folding models.
Pay attention to weight and mobility
Some massage tables are designed to hold around 350 kg. This may seem strange, but keep in mind that the table takes on the load from the mass of not only the patient, but also the doctor. Such models are especially relevant for doctors with an impressive build. On the other hand, sometimes a massage therapist needs to go to the patient’s home. In this case, mobility comes to the fore.
 Today there are many options for lightweight models that are easy to transport and put into working condition. One of the best options in this sense is US Medica Super Light, weighing only 10.68 kg. When folded it is very compact. The transformation system is convenient and reliable: the model unfolds without any effort and very quickly. There's also a removable headrest with a face cutout. And in addition - smooth stepless adjustment of the angle of inclination, plus the ability to change the height of the table within 60-80 cm.
Today there are many options for lightweight models that are easy to transport and put into working condition. One of the best options in this sense is US Medica Super Light, weighing only 10.68 kg. When folded it is very compact. The transformation system is convenient and reliable: the model unfolds without any effort and very quickly. There's also a removable headrest with a face cutout. And in addition - smooth stepless adjustment of the angle of inclination, plus the ability to change the height of the table within 60-80 cm.
Pay attention to the following features of mobile massage tables:
- They have legs with plastic attachments, so the floors are not damaged.
- When assembled, they are so compact that they can be easily transported even on public transport.
- The legs in these models allow you to secure the table even on uneven floors. An adjustment system is provided for this.
Among the stationary options, it is worth highlighting Olimp and Bali from US Medica. American designers have learned to combine functionality, ergonomics and image characteristics. However, their price is higher.
Massage tables for pregnant women
 Previously, some types of massage were not available to pregnant women. During this period, a woman’s spine experiences constant stress. However, American developers managed to find a solution to the problem. The US Medica Panda model is suitable for comfortable acupuncture, lymphatic drainage, reflexology and many other procedures.
Previously, some types of massage were not available to pregnant women. During this period, a woman’s spine experiences constant stress. However, American developers managed to find a solution to the problem. The US Medica Panda model is suitable for comfortable acupuncture, lymphatic drainage, reflexology and many other procedures.
Externally, the model looks extremely concise and strict, which was the result of careful mathematical modeling. Even in lighter models - Samurai or Master - the design and material allow them to withstand high loads (220-250 kg). We are talking about dynamic, or active, load, which during procedures exceeds static. The models are also equipped with convenient bags-covers where you can store the assembled structure.
Note! The roller joints use a special polymer that does not break or crack under any circumstances, and the transformation occurs almost silently.
Factors that will help you make a choice
Let's summarize. Here are factors to help you make a smart choice:
- First of all, the convenience and comfort of the patient.
- Strength of the material. Noticeable at first glance Beautiful design, however, it is more important to make sure that the material is not prone to abrasion and does not lose its original appearance over long periods of use.
- Even the most small parts are distinguished by impeccable environmental friendliness.
More specifically, the upholstery should be “breathable”. A classic example is high-strength artificial leather. Its color can be selected in accordance with the design of the office. And to ensure comfort, conscientious manufacturers use gas-filled foam materials - foam rubber and polyurethane, which are both elastic and soft. Great option premium class - Arpatek. It is used for upholstery of seats in luxury cars. These parameters were taken into account by US Medica and Yamaguchi.
It is generally accepted that classical massage, called Russian throughout the world, is one of the most natural, natural and effective means of training athletes, improving health, preventing and treating various diseases, as well as improving the aesthetics of the human body. At the same time, we must not forget that performing Russian massage for a whole working day or shift, the duration of which when working with athletes can reach 12-15 hours a day, is tiring, even for trained experienced specialists, hard physical labor, the organization of which requires full and comprehensive scientific justification. However, despite the obvious relevance of this problem, until recently, the range of issues related to increasing the performance and preventive prevention of professionally caused diseases of massage therapists was not studied at the proper level, and therefore, there were no scientifically based and clearly formulated recommendations for rational organization of labor of specialists in this profile. As our analysis of domestic and foreign textbooks and teaching aids on classical massage revealed, in most cases, the authors’ statements on this issue are of an unfounded subjective-empirical, often mutually exclusive nature, and moreover, often completely contradict modern views of biomechanics, requirements occupational health and ergonomics. This state of affairs, completely unacceptable for a scientific and educational discipline, prompted us to undertake our own comprehensive research, the purpose of which is to develop, substantiate and introduce into the pedagogical process and practical sphere of massage extremely accurate, effective and accessible recommendations for maintaining health and increasing performance massage therapists
The optimally adjusted one, which is the main element of equipment for Russian massage rooms, plays a decisive role in the ergonomics of the massage therapist’s workplace. The correct adjustment of its size largely determines the working conditions of the massage therapist, i.e. will his working posture be ergonomically rational and functionally comfortable, or, on the contrary, forced, leading to rapid fatigue. Our critical analysis large quantity textbooks and manuals on classical massage - currently, a whole spectrum simultaneously coexists, including diametrically opposed opinions about the optimal height of the massage table. The authors' recommendations on this issue have fairly wide limits: from 50 (or at the level of the knee joints) to 90 cm (Table 1), while most publications indicate only a certain range of possible sizes (50-70 or 70-90 cm) , without any further explanation. Methods for adjusting the height of the table taking into account the height and length of the massage therapist’s arms are extremely rare, and they often contradict the principles and standards of ergonomics and occupational hygiene.
As is clearly seen from Fig. 1, in relation to the anthropometric dimensions of the human body, the range of 40 centimeters is a significant value, suggesting working postures that are completely different in design, some of which can be even based on formal characteristics (Gorshkov S.I., 1979; Strelkov Yu.K., 2003) classified as forced, inconvenient. And finally, there is an Industry Safety Standard for physical therapy departments and rooms - OST 42-21-16-86 SSBT, which clearly defines that the height of the massage table should be 80 cm, length 1.95-2.00 m, width 0.65 cm, the ergonomic justification for which we were unable to find in the available literature.
In the process of research conducted on the basis of the Russian state university physical culture, Sports and Tourism (Moscow), we studied 4 variants of the “standing” working posture, which were modeled by adjusting the height of the massage table in accordance with the individual anthropometric data of each of the subjects:

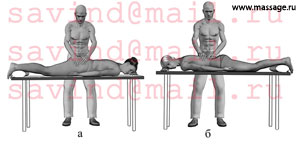
Rice. 2. Working postures modeled during the study (explanations in the text).
Working Pose 1 (RP-1) – table at the level of the knee joints (Fig. 2-a);
- Working Pose 2 (RP-2) – table at the level of the finger point, i.e. the hand is freely lowered, the fingers are fully straightened and touch the bed of the table (Fig. 2-b);
- Working Pose 3 (RP-3) – table at the level of the phalangeal point, i.e. the hand is freely lowered, the fingers are clenched into a fist and touch the back of the table bed (Fig. 2-c);
- Working Pose 4 (RP-4) – table at the level of the styloid process of the radius (Fig. 2-d).
Thus, we evenly covered the entire range of recommendations on the size of the massage table. As a standard workload, the subjects performed a 45-minute session of general hygienic massage according to the method of A.A. Biryukova (2006). Using the multifunctional computer electrophysiological complex “I-330-C2+” (J+J Engineering, USA), we recorded: heart rate (HR), depth and frequency of breathing, bioelectrical activity of the muscles directly involved in maintaining working postures (sacrospinous , gluteus maximus, biceps femoris, gastrocnemius, trapezius, deltoid, biceps femur). At the same time, goniometric and photogoniometric measurements, psychophysiological testing and a questionnaire survey of subjects, as well as pedagogical observation were carried out. In total (to date), more than 150 subjects from among students and participants of massage courses at the Russian State University of Physical Culture and Technology took part in the research, which allows us to reasonably assert the statistical reliability of the data obtained.

Rice. 3. Optimal working posture (perpendicular starting position).
The results of our study convincingly proved that from the point of view of physiology, biomechanics and ergonomics, the most rational options to perform Russian classical massage, the specialist worked in RP-2 (table height at the level of the finger point) and RP-3 (table height at the level of the phalangeal point), in which the torso tilt did not exceed 15-20° (Fig. 3). Comparative analysis showed that the bioelectrical activity of muscles in RP-2, -3 had the smallest differences from the data recorded in a calm, comfortable “standing” position (Fig. 4).

Rice. 4. The amplitude of bioelectrical activity of some skeletal muscles when working in an optimal position and in a comfortable “standing” position.
It is fundamentally important that during the entire 45-minute session, the amplitude and frequency spectrum of electromyographic signals did not change significantly, as evidenced by (Moikin Yu.V. et al., 1987; Rozhentsov V.V., Polevshchikov M.M., 2006 ) about the absence of even primary signs of neuromuscular fatigue, that is, about a relatively low load on the skeletal muscles fixing these postures.
In RP-2,-3, working hyperventilation was carried out mainly due to an increase in the depth of breathing by 210±24% (compared to rest) and a slight increase in the respiratory rate by 2-4 cycles/min, i.e. according to the most advantageous option for mobilizing external respiration reserves during cyclic physical work (Fig. 5).

Rice. 5. Pneumogram (graphic registration of amplitude and frequency parameters of movement chest, reflecting the dynamics of respiratory movements) during massaging in the optimal working position.
The breathing was rhythmic. A joint analysis of pneumo- and electromyograms showed that in these working postures the respiratory act was organically inscribed “into the fabric” of the movements performed by the hands, forming a single ensemble with it - a dynamic stereotype.
With the beginning of the massage, heart rate increased compared to the pre-working state (68±6 beats/min) by 70.5% (up to 116±11 beats/min) and remained within these limits until the end of the session.
According to the questionnaire survey, RP-2, -3 were characterized by the subjects not only as somatically (physically) comfortable, but also as the most convenient for performing massage techniques. Photogoniometric measurements showed that the subjective comfort of performing techniques noted by massage therapists has a well-defined biomechanical foundation.
Firstly, in these working poses a biomechanically favorable spatial arrangement of the specialist’s torso, the links of his arms and the massaged area was created relative to each other. The shoulder-forearm-hand of the massage therapist and the massaged area were arranged in descending order downwards. On average, the angle of flexion in the shoulder joint (measured in accordance with the international methodology - SFTR) was 20-25°, shoulder abduction from the body did not exceed 15-20°, elbow flexion 20-30° (Fig. 6).

Rice. 6. The relative position of the links of the biokinematic chain of the torso-shoulder-forearm-hand of the massage therapist in the optimal working position.
As shown by the results of electromyography, such a mutual position required optimal expenditure of muscle energy to hold the arms in the working position and made it possible to fully relax the muscles that were not involved in performing the entire technique or its individual phases (Fig. 7).

Rice. 7. Electromyograms when a massage therapist performs a “double circular kneading”: t – period of performing one pass of a “double circular kneading”. The main working movement “forward movement of the arm” is accomplished due to the activity of the triceps brachii. Activity of the biceps brachii is required only to return the arm to its original position.
To use a term from labor physiology, working muscles had micro-pauses of rest, which significantly delayed the onset of their local fatigue.
Secondly, at an optimal table height, the massage therapist’s hand, in contact with the patient’s body, occupies the most advantageous position in relation to the forearm. Normally, flexion of the fingers is accompanied by simultaneous extension in the wrist joint, within 20-30° (Fig. 8).

Rice. 8. Stabilization of the wrist during finger movement. From the point of view of biomechanics, this synkinesis is largely due to the need to compensate for the passive insufficiency of the finger extensors (Mateev I.B., Bankov S.D., 1981).
Such synkinesis is deeply recorded in the central nervous system a person, and is biologically expedient, since it directs the plane of the palm against the object to be captured. The strength of the hand grips reaches its maximum values when the extension angle in the wrist joint is 30-40°. If the hand is in a neutral position or, which is much worse, in a flexion position, then the mobility of the fingers in the interphalangeal joints significantly worsens, and the effective area and strength of most types of grips decreases (Aruin A.S., Zatsiorsky V.M., 1989 ; Mateev I.B., Bankov S.D., 1981). It is on this biomechanical pattern that most techniques for disarming the enemy in various martial arts are based. In addition, as studies by A.S. have shown. Aruina and V.M. Zatsiorsky (1989), G.N. Mazunina et al. (1967), Yu.V. Moikina et al. (1987), with long work with excessive flexion or extension of the hand, the risk of developing occupationally-related pathological processes in various anatomical structures of the hand and forearm sharply increases: soft tissues, articular surfaces, ligaments and tendons.
The essence of performing ordinary, double ordinary, double ring kneading, double bar - the most technically complex types of Russian massage techniques and at the same time occupying from 60 to 80% of the total session time, lies in grasping with the hands, lifting from the bone bed, squeezing and stretching / torsion of the muscle tissue of the massaged area of the patient’s body.
Therefore, with very minor reservations, we can assume that performing the above types of kneading is nothing more than repeated cyclic repetition of various variations of the palmar (open) grip of the hand (Fig. 9) with a compression force of the massaged tissue of about 4-5 kg (Eremushkin M .A., 2004).

Rice. 9. Palmar (open) grip of the hand.
According to goniometric and photogoniometric measurements, when performing the above types of kneading in RP-2, -3, extension in the wrist joint, on average, was 15-30° (Fig. 10), that is, it was the most biomechanically advantageous, which in many ways and predetermined subjective convenience and good technique for performing most techniques.

Rice. 10. Biomechanically favorable mutual position of the biokinematic pair forearm-hand when performing types of kneading. 
Rice. eleven. General form working position – 4, table at the level of the styloid process of the radius.
When modeling RP-4 (Fig. 11) (massage table at the level of the styloid process of the radius), the position of the subjects’ torso was almost vertical (inclination less than 10°), but the arms were constantly in a forced elevated position.

Rice. 12. Forced raised position of the arms in a working position – 4: a – position of the biokinematic pair shoulder-forearm in relation to the body; b – relative position of the forearm-hand biokinematic pair when performing types of kneading.
The angle of flexion in the shoulder joint (Fig. 12,a) exceeded 50°, and abduction of the shoulder from the body was 25-30°, which, compared to RP-2,-3, not only increased the amplitude of the bioelectrical activity of the trapezius muscle by more than 5 times , deltoid muscle by 4-6 times and biceps brachii muscle by 2 times, but also increased the activity of the sacrospinalis muscle by 82±12% and the biceps femoris muscle by 90±8% (Fig. 13).

Rice. 13. The amplitude of bioelectrical activity of some skeletal muscles when working in the optimal position and working position is 4.
Keeping the arms in a raised position limited the excursion of the chest, making it difficult for the massage therapist to operate the external respiration apparatus. The depth of breathing was 42% less, and the frequency was 26% higher than similar indicators in RP-2, -3, i.e. breathing was shallow and rapid (Fig. 14).

Rice. Fig. 14. Pneumogram when performing double circular kneading: a – in the optimal working position, b – in the working position – 4 with arms raised high.
This fact also has a very specific physiological and biomechanical explanation. Gas exchange in the body is carried out thanks to rhythmic respiratory movements by changing inhalation (inspiration) and exhalation (expiration). At rest and during light work, respiratory movements are provided by the respiratory muscles themselves. In this case, the greatest activity is observed during inhalation in the diaphragm and intercostal muscles, and exhalation is performed largely passively, due to the elastic forces that arise when the chest and lungs expand during inhalation. With significant physical activity, auxiliary respiratory muscles come into play - on inhalation, the trapezius and rhomboids, pectoralis major and minor, sternocleidomastoid, back extensors and some others, and on exhalation, the abdominal muscles. It should be taken into account that in RP-4, most of the listed muscles developed significant static activity to keep the arms in a raised position, and some also performed dynamic work when performing techniques. Thus, double and even triple load on these muscles became a very significant factor limiting lung ventilation.
Increased muscle activity and functional tension of the external respiration apparatus naturally affected the activity of the cardiovascular system. In RP-4, the heart rate was 35.3% higher than in RP-2, -3, which in absolute value was 140±11 beats/min.

Rice. 15. Zones of localization of discomfort sensations (shaded with a grid) when massaging in a working position - 4 (according to a questionnaire survey conducted directly during a 45-minute test massage session).
Subjectively, the subjects assessed this working position as tiring (Fig. 15) and inconvenient for performing most types of techniques, primarily various types of kneading, which was also, in the most direct way, related to the biomechanical patterns we discussed above.
Firstly, keeping the arms in a constantly raised position did not allow the large muscles of the arms: the biceps and triceps brachii to fully relax in micropauses, which is quite contrastingly seen when comparing the electromyograms recorded in RP-2 (Fig. 7, a) and RP- 4 (Fig. 7,b).
Secondly, photogoniometric measurements revealed that when performing various types of kneading in RP-4, the hand in relation to the forearm was in a neutral or even slightly bent position of 5-10° (Fig. 12), which worsened the mobility of the finger joints and strength indicators of distal muscles.

Rice. 16. General view of the working position – 1, table at the level of the massage therapist’s knee joints.
The most irrational of all the modeled working postures was RP-1 (table height at the level of the knee joints), in which the torso tilt reached 30°-45° (Fig. 16), which was 2-3 times higher than the ergonomic norm of 15°, maximum permissible GOST 12.2.033-78 " Workplace when performing work while standing.”
Practice shows that a correct understanding by massage therapists of the essence of this ergonomic norm is exclusively an important condition for adequate self-control during work and modeling the most comfortable and safe conditions labor, so we will consider this issue in more detail.
With relatively small inclinations of the torso and head, a certain part of the load on the spine is compensated by increasing the tension of the muscles of the back (mainly the rectus abdominis) and abdomen (rectus abdominis and its synergists) (Fig. 17).

Rice. 17. The spinal motion segment of a vertically standing person is like a lever of the first kind (balance lever) with unequal shoulders. The fulcrum of the lever is the nucleus pulposus of the intervertebral disc, and the balance of the system is achieved due to the activity and elastic-viscous properties of the skeletal muscles of the back and abdomen: 1 - iliopsoas muscle, 2 - rectifier spinae muscle, 3 - quadratus lumbar muscle, 4 – straight abdominal m., 5 – oblique abdominal m.
In this case, the stability and stability of the spine is ensured not only with the help of intervertebral discs, joints and a fairly powerful ligamentous apparatus, but also due to the activity of skeletal muscles. According to the famous domestic specialist in the field of vertebrology, physical rehabilitation and therapeutic physical culture, Professor V.A. Epifanova (2004): “The muscles of the trunk are not only a motor element, but also a structural element, without which the strength of the spine differs little from zero.” However, the biomechanics of the human body is such that when the body is tilted more than 15-20° from the vertical, these skeletal muscles cease to provide active support to the passive structures of the spine (Fig. 18).

Rice. 18. Compression (in Kg) transferred by the lumbar intervertebral discs, depending on the person’s posture (according to Slynchev P. et al., 1978).
In this situation, the main part of the load is redistributed to the intervertebral discs and joints, and their ligamentous apparatus, which are not functionally designed for long-term performance of such a supporting function. Over time, such mechanical impact can cause tissue overstrain syndrome, which manifests itself in compensatory compaction, adhesion, and fibrosis of the cartilaginous and ligamentous structures of the spine. First of all, the intervertebral discs suffer, which lose their elastic and shock-absorbing properties, microdamages accumulate in them, creating conditions for deformation and subsequent violation of their integrity. It should be taken into account that “turning off” the back and abdominal muscles from the process of stabilizing the posture only concerns their support of the spine and does not lead to a reduction in the load on the skeletal muscles themselves. On the contrary, with body tilts exceeding 15-20°, the load on the muscular system increases sharply (Aruin A.S., Zatsiorsky V.M., 1988; Epifanov V.A., 2004; Gorshkov S.I., 1979; Levit K. et al., 1993), which was confirmed by our own studies.

Rice. 19. The amplitude of bioelectrical activity of some skeletal muscles when working in an optimal position and working position is 1.
Analysis of electromyograms showed (Fig. 19) that the amplitude of the bioelectric activity of the muscles of the back and legs was already initially higher than in RP-2, -3 (sacrospinous by 4-4.5 times, gluteus maximus by 1.5 times, biceps femur by 2-2.5 times, gastrocnemius by 1.2 times), and its dynamics are characteristic of the electromyographic picture of pronounced deep fatigue during static efforts (Fig. 20).

Rice. 20. Electromyographic picture of pronounced deep muscle fatigue during static efforts during massaging in a working position - 1 and its transformation with the development of muscle fatigue. Subject K., male, 26 years old, work experience as a massage therapist for 3 years.
The continuous increase in the amplitude of the bioelectrical activity of the sacrospinalis muscle (phase of “compensated fatigue”), which continued during the first 30 minutes of massage, was then replaced by a sharp decrease in the last third of the session (phase of “decompensated fatigue”). In parallel with this, there was an increase in the activity of the gluteus maximus and biceps femoris muscles, which initially played an auxiliary role in maintaining an inclined position of the body and gradually took on the main load. Visually, this process manifested itself as a transformation of posture. At the beginning, despite the deep tilt, the contour of the back was quite even, and the legs were slightly bent at the knees and hip joints. With the development of muscle fatigue, i.e. As the activity of the sacrospinalis muscle decreased, the contour of the back became more and more rounded, and the legs almost completely straightened. In addition, as fatigue of the muscles of the back and legs increased, the subjects often stabilized the balance of their body by relying on one of their hands or knees, involuntarily trying to at least temporarily reduce the load on the muscles. Significant tension in the muscles responsible for maintaining a working posture was subjectively assessed by the subjects as a feeling of fatigue, numbness, aching, burning and pain in the lower back, buttocks and thighs (Fig. 21).

Rice. 21. Zones of localization of discomfort sensations (shaded with a grid) when massaging in a working position - 1.
Increased muscle activity forced the cardiovascular system to function more intensely than in RP-2,-3. The heart rate already at the 1st minute of massage was 156±4 beats/min (+58.9%), and by 30-45 minutes it increased to 168±4 beats/min (+76.5%). The bent position of the body made it difficult for the external respiration apparatus to operate. The pneumogram showed that in RP-1 the breathing of the subjects was not only shallow and rapid (the depth of breathing is 52% less, the respiratory rate is 42% higher than similar indicators in RP-2, -3), but also irregular, with delays of 4- 6 seconds (Fig. 22).

Rice. 22. Pneumogram when performing double circular kneading in a working position - 1. Small fluctuations in the amplitude of the signal in the area indicated in the figure as “breath holding” are due to the rhythmic contraction of the muscles of the chest and back when performing techniques, which was recorded by the equipment as a change in the size of the chest.
However, unlike RP-4, the main role in complicating the operation of the external respiration apparatus was played not by the forced position of the arms, but by excessive flexion of the torso, which led to limited mobility of the ribs and mechanical pressure on the diaphragm of the abdominal organs.
At the same time as the above, it is necessary to take into account that the bent position of the torso also leads to compression of the abdominal and pelvic organs, as well as to obstruction of blood circulation in the portal vein (v. portae). According to L.K. Arzhelas (1927) - according to our data, probably the only domestic specialist who studied the problem of professional morbidity among massage therapists, long-term exposure to the body of these two factors can cause the development of congestion, varicose veins, constipation, hemorrhoids, weakening of the pelvic floor muscles, and in women – various gynecological pathologies.
Thus, based on the generalization and analysis of the data obtained, we recommend the following method for determining the optimal (i.e., most suitable for a given person) height of the massage table: the specialist needs to stand close to its edge, the feet and knees of fully straightened legs should touch each other friend, keep your torso straight, turn your shoulders, lower your arms freely (Fig. 23).

Rice. 23. Definition optimal height massage table in accordance with the individual anthropometric data of the massage therapist.
The height of the table is within optimal limits if its surface is located in the range limited by the following anthropometric points (landmarks): below - finger point (tip of the nail phalanx of the 3rd finger), above - phalangeal point (back side of the middle phalanges of the fingers clenched into a fist) .
In accordance with the most current data at the moment on the static and dynamic anthropometric signs of the human body of the inhabitants of the European part of Russia (Strelkov Yu.K., 2003; Strokina A.N., Pakhomova V.A., 1999), as well as the results of our own anthropometric measurements (Fig. 1), the average height of men is 175 cm (height of the finger point above the floor - 66 cm, phalangeal point - 77 cm), and women - 163 cm (height of the finger point above the floor - 63 cm, phalangeal point - 73 cm ). Based on this information, focused on Russian market Manufacturers of specialized furniture for massage rooms must produce massage tables, the height of which can be adjusted no less than in the range of 60-80 cm. If this condition is met, more than 90% of massage therapists (men and women) will have the opportunity to work in optimal conditions.
We would like to draw the special attention of all competent specialists to the need to make ergonomically sound adjustments to the Industry standard for organizing massage in medical institutions OST 42-21-16-86 SSBT, since the table height of 80 cm indicated in it is too high not only more than for 95% of women (80 cm approximately corresponds to the level of the styloid process of the radius), but is also the upper limit of the optimal range for men.
To more accurately adjust the table height, it is advisable to be guided by the following criteria.
Rice. 24. Options for adjusting the height of the table depending on the transverse sagittal dimensions of the massaged body: a – table at the level of the finger point (lower limit of the optimal range); b – table at the level of the phalangeal point (upper limit of the optimal range).
In the case when it is necessary to perform techniques with high intensity (i.e. depth) of impact on tissue: massaging a person with developed muscles or significant fat deposits (Fig. 24, a), it is recommended to adjust the height of the table at the level of the finger point. The surface of the massaged area will be located slightly lower than the general center of gravity of the massage therapist’s body, which allows increasing the intensity of the impact not only by increasing muscle effort, but also through the effective use of weight and inertia of torso movement. It is important that in this case the specialist does not lose balance (i.e. does not fall on the patient) and can quite accurately control the applied efforts and intensity of the impact.

Rice. 25. When massaging a child whose body size is much smaller than that of an adult, the height of the table should be at the level of the phalangeal point (the upper limit of the optimal range).
If the session does not involve performing techniques with great strength and intensity: some private massage techniques for diseases, massage of a child (Fig. 25), or the transverse sagittal dimensions of the patient’s body are small (Fig. 24, b), then it is more advisable to choose the height of the table at the level of the phalangeal point so that the tilt of the body is minimal.
Another important ergonomic parameter of a massage table is its width. The table should be wide enough (spacious) for a comfortable, absolutely relaxed position of the patient on it, but at the same time it must be taken into account that the excessive width of the bed forces the massage therapist to work with a deep torso tilt and outstretched arms, in fact, reducing to zero all efforts to optimize the work poses due to precise adjustment of the table height (Fig. 26).

Rice. 26. Despite the precisely adjusted height of the table, its overly wide bed forces the massage therapist to work in an uncomfortable working position.
Equipment manufacturers are trying to find a compromise between these two requirements, giving the surface of the table bed a complex concave shape or providing transformable, removable palm rests and armrests.
Based on the results of our own research, practical experience work, as well as anthropometric data of Russian residents (Strelkov Yu.K., 2003; Strokina A.N., Pakhomova V.A., 1999), we recommend a table width of 55-65 cm.
We hope that the results of our research will be useful for a wide range of people whose profession is related to massage: teachers of educational institutions and courses, practicing massage therapists and, of course, for those who have just begun to study it. In addition, we believe that the data presented in this publication will be of interest to managers of various institutions and organizations (medical, health, sports, SPA industry and beauty salons) that provide massage services, as well as for manufacturers of massage equipment and furniture .
Table No. 1.
| 1. | Latoguz S.I., 2001, 2007 | The height of the massage table should be 5 cm above the massage therapist’s knee joint (about 50 cm) |
| 2. | Poghosyan M.M., 2002 | 50-70 cm |
| 3. | Vasichkin V.I., 1991, 1993 | 50-70 cm |
| 4. | Kondrashev A.V., Khodarev S.V., Kharlamov E.V., 2005 | 50-70 cm |
| 5. | Fokin V.N., 2002 | 60-80 cm |
| 6. | Efimenko P.B., 2001 | Standing at attention, hands at your sides, the ends of straightened fingers should touch the surface of the table (about 66 cm) |
| 7. | Makarov V.A., 1975 | 70 cm |
| 8. | Sarkizov-Serazini I.M., 1963 | 70 cm |
| 9. | Tyurin A.M., Vasichkin V.I., 1986 | 70 cm |
| 10. | Leontiev A.V., 2004 | In a standing position, arms straightened and lowered down, the massage therapist should touch the surface of the table with the middle phalanges of the fingers (about 70 cm) |
| 11. | Kramarenko V.K., 1953 | 70-75cm |
| 12. | Dunaev I.V., 2000 | In a standing position, arms are straightened and lowered down, the fingers gathered into a fist should touch the surface of the table with the back of the main phalanges (about 75-77 cm) |
| 13. | Kunichev L.A., 1984 | 70-75 cm, |
| 14. | Zabludovsky I.Z., 1903 | 77 cm |
| 15. | Dalikho V.A., Hase H., Krauss G., Reichert H., Schumann N.L., 1983 | 75-80cm, height should be stable for stability reasons |
| 16. | Belaya N.A., 2001 | 80 cm |
| 17. | Verbov A.F., 1966 | 80 cm |
| 18. | OST 42-21-16-86 SSBT | 80 cm |
| 19. | Shterengerts A.E., Belaya N.A., 1992 | 70-90 cm |
| 20. | Dubrovsky V.I., 2001 | 70-90 cm |